Recently, Cell Symposia celebrated the 10-year anniversary of the seminal publication on inducible pluripotent stem cells (iPSCs). An audience of scientists from academia, biotech and pharma gathered to celebrate Drs. Yamanaka and Takahashi’s work and to discuss the future of iPSCs as therapeutics and in research. In addition, the Gladstone Institute celebrated the 2016 Yamanaka-Ogawa Prize, awarded to a leading developmental biologist Dr. Doug Melton. Here, I’ll share some of the highlights with you and hope to begin our discussion on how the research and development of iPSCs continues to contribute to new discoveries and therapeutics developments.
Dr. Shinya Yamanaka at the Cell Symposia: Dr. Yamanaka detailed the trials and tribulations of his institute’s collaborative efforts (with the RIKEN Center for Developmental Biology, Japan) in the pioneering iPSC-derived RPE clinical trial for age-related macular degeneration. Patient was a 70-year-old woman who suffered from exudative (wet-type) age-related macular degeneration and she became the world’s first recipient of human iPS-derived RPE transplantation. Somberly, Yamanaka explained why he, as the director of the institute, had to make the final decision to discontinue the clinical trial before proceeding onto the second patient. Here are his main points:
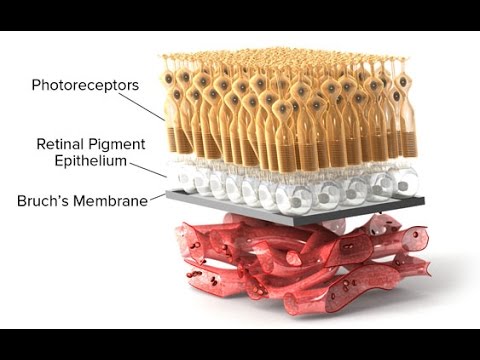
- Autologous iPSCs-derived Retinal Pigment Epithelial (RPE) cellular therapy involves deriving retinal support cells, RPEs, from the patient’s own skin samples using stem cell reprogramming technologies. The manufacturing and quality-control process takes about a year to complete. Thus, it takes 1-2 years from the start of the process to until the cells are ready to be used in surgery.
- “[The] Cost would be too high,” Dr. Yamanaka noted. He estimated that it would cost around $500,000.00 (USD) or more per treatment.
- It took over 50 scientists at the institute nearly 2 years to engineer a sufficient number of cells and to make sure that the cells were safe for patient-use. Yamanaka admitted he was worried that a patient’s’ prognosis would change between the start of the process and the final surgery.
- From a safety point of view, the first patient’s cells passed safety requirements during the clinical trial. But when the procedure was repeated for the second patient, an unexpected mutation was identified during the manufacturing process, a copy number variation, CNV 15q11.2. This finding warned scientists of the risk in generating patient-derived cells for therapy and of the need for higher quality control measures.
{kind=link}
If autologous iPSC cell therapy is too expensive, is allogeneic cell therapy an alternative solution? He mentioned that the most critical part is to identify a sufficient number of donors that would satisfy the general population’s needs and prevent immune rejections. As an example, he estimated that for around 90% of Japan’s population, approximately 250 HLA homozygous donors would be needed. So far, with the help from the Japanese Red Cross, 14 donors have been identified.
In closing, he encouraged scientists to use iPSCs reprogramming technologies to explore disease mechanisms, particularly in disease modeling, to discover novel features and characteristics for drug development. As an example, he presented a project from his lab on the mechanisms of cartilage repair (Yamanaka Lab, unpublished data) which benefitted from using iPSC-derived cell types. Furthermore, he and his team are searching for chemical molecules that could be used as drug candidates and are learning about novel mechanism for human cartilage formation.
Dr. Doug Melton at the Ogawa-Yamanaka award ceremony: As one of the pioneers in the field of regenerative medicine, Dr. Melton’s passion for finding treatments for diabetes has been propelling the field forward for a number of years. Engineering human stem cells into pancreatic beta cells that secrete insulin has been the ultimate goal of his laboratory. To be able to achieve this goal in human patients will be ground-breaking for diabetes patients worldwide, especially for those who live with Type 1 Diabetes. There are numerous milestones along the road towards understanding the biology of pancreas and beta cells. The most outstanding achievement is simply that, approximately 20 years ago, it was not possible to discuss treatment potentials where patients could receive their very own beta cells to secrete insulin as a cure for the disease.
Moving forward, his lab, in partnership with two biotech startups, Semma Therapeutics and Viacyte, face challenges some of which he explained including:
- Efficiency of generating beta cells for the patient needs improving so that it will require less time in manufacturing pure populations of human beta cells. Furthermore, a cost of about $1million (USD) per patient (per treatment) has been projected.
- Controlling specific cell types generated during the manufacturing process will be needed in the future in order to engineer patient-specific treatment.
- Immunogenicity is a great challenge of for patients. Immune reactions can be triggered to reject treatment.
Looking forward: There are significant scientific and technical challenges ahead in providing iPS-derived cell products as therapeutic products for patients (aka Regenerative Medicine). As a set of discovery tools, iPSCs and their derivative cell types provide important resources for all drug discovery scientists. My hope is that the international iPSC community will discover new drug candidates and biological insights to further understand the unique mechanisms of different human diseases in the coming years.
Thank you to the people at Cell Stem Cell and the Gladstone Institute for organizing this year’s events. See you all next year!